| ABOUT
SNORING
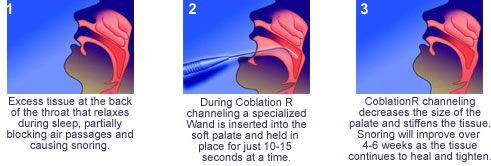
For further help with any snoring problems you may have, click on the Questionaire links at the bottom of this page. Until recently, snoring has been largely ignored by medical science. While the snorer sleeps undisturbed, the sleepless listener develops the chief symptoms of a disease that afflicts also the unafflicted. Snoring is more widespread then generally believed. Up to 45% of adults snore occasionally, while 25% are habitual snorers. Snoring is more common in males, increases with age in both sexes and is 3 times more common in the obese. The majority of people over the age of 65 snore. Rarely does the snorer himself seek medical attention. For reasons that are not understood, the snorer does not hear himself regardless of the loudness. Sounds in excess of 80dB have been recorded. The snorer usually comes at the insistence of a bed partner or former partner. Currently, the general public and much of the medical profession are unaware of the potentially serious disorders associated with snoring. Complaints will be related to the loudness and frequency. Since occasional, light snoring causes no ill effect, patients such as these probably need no treatment. However, rarely do these people seek medical attention. The social embarrassment caused and felt by these people is never to be ignored and is not an uncommon cause for marital disharmony. Snoring and sleep apnoea are related. Snoring increases in severity over time and can progress to sleep apnoea. Recent sleep studies have linked snoring to systemic and pulmonary hypertension, right heart failure, cor pulmonale, secondary polycythemia and cardiac arrhythmias. During sleep severe snorers may experience apnoea, oxygen desaturation, carbon dioxide retention and nocturnal pulmonary and systemic hypertension. Causes Treatment Radiofrequency Palatoplasty (COBLATION R) is a revolutionary new treatment now available. The tissue in the soft palate and uvula are reduced and stiffened without the pain associated with conventional laser assisted surgery. This is a fast and effective way to reduce uvulopalatal snoring, without the pain and inconvenience associated with traditional surgical techniques. It is performed in an out-patient setting under local anesthesia. The procedure itself takes less than 15 minutes of surgical time. The unique design of the needle electrode and the automated control of the tissue temperature protects the mucosa. After the procedure, most patients take only over-the-counter analgesics They will usually experience a reduction of snoring within six to eight weeks. Non- surgical approaches include weight loss and other lifestyle modifications. |
 |
  |
INJECTION SNOREPLASTY This is a new procedure for the treatment of snoring. It is safe, relatively painless and inexpensive. It is easy to perform in the rooms and is often just as effective as the more painful and previous costly surgical procedures. Many treatments for snoring have been devised over the years. Initially the uvulopalatopharyngoplasty (UPPP) was devised as a means of decreasing palatal vibration by extensively resecting the uvula, soft palate and tonsils. Its main indication was for the treatment of sleep apnoea. Modifications to these procedures include the laser assisted uvulopalatoplasty (LAUP) and radio frequency uvulo palatoplasty (RFUP) and radio frequency palatal ablation (RFPA).These involve shrinking of the soft palate and uvula in the hopes of cutting down palatal flutter and thus reducing snoring. All these procedures enjoy some degree of success, ranging from 40% - 90% with a recurrence rate of more than 20%. Obesity was a major cause of failure in each of these procedures. Other surgical procedures directed at the nose in the hopes of improving nasal airway can certainly improve snoring but only is nasal obstruction is the primary cause. These procedures include a septoplasty, turbinate reduction and if necessary endoscopically directed sinus procedures. Other non-surgical procedures have been developed which at best provide temporary relief. These include dental appliances, lubricating sprays and external nasal strips. After studying the movement of the palate in snoring it was thought that by inhecting a substance into the palate, which would result in palatal stiffening by causing scarring and thus reduce the amount of snoring. The injection snoreplasty was developed after extensive research in the USA. Initial success rate has been in the region of about 90% with the recurrence rate of about 20%. THE PROCEDURE Over the next week the area where the agent has been injected will turn white and with slough off leaving a small ulcer. This ulcer then contracts and forms a scar, which stiffens the palate. Initial snoring in the first three weeks is worse but over the time it decreases and by the sixth week one is able to get a reasonable idea of the success rate. Repeat injections are sometimes necessary. RESULTS It must be noted that prior to doing the procedure, a full ENT Specialist evalutation must be undertaken. This is to determine the suitability of the procedure and the cause of the snoring and to assess any contributing causes to the snoring. |